QUICK ANSWER
A presenting with confidence course is worth buying when it trains the specific patterns of senior-level rooms — calmness under scrutiny, voice and breath under pressure, and recovery from the visible signs of nerves — rather than generic stage fright. Evaluate any course on four dimensions: who the audience is built for, what is actually trained, the format, and whether the work transfers to the specific rooms you present in. Most courses fail on the first dimension, which is why the rest never lands.
JUMP TO
What you are actually buying ·
Four dimensions to evaluate ·
Red flags to watch for ·
What good looks like ·
Making the decision ·
FAQ
Folake had been searching for a presenting with confidence course online for three weeks before she bought one. She is a divisional director at a UK insurer, presenting to the executive risk committee roughly twice a quarter. The nerves were not a daily feature of her job. They were a feature of those specific mornings — the rooms where one wrong sentence under questioning could cost her credibility for the rest of the year. She bought the highest-rated course she could find, finished it in four evenings, and felt, by her own description, “more polished but no calmer.”
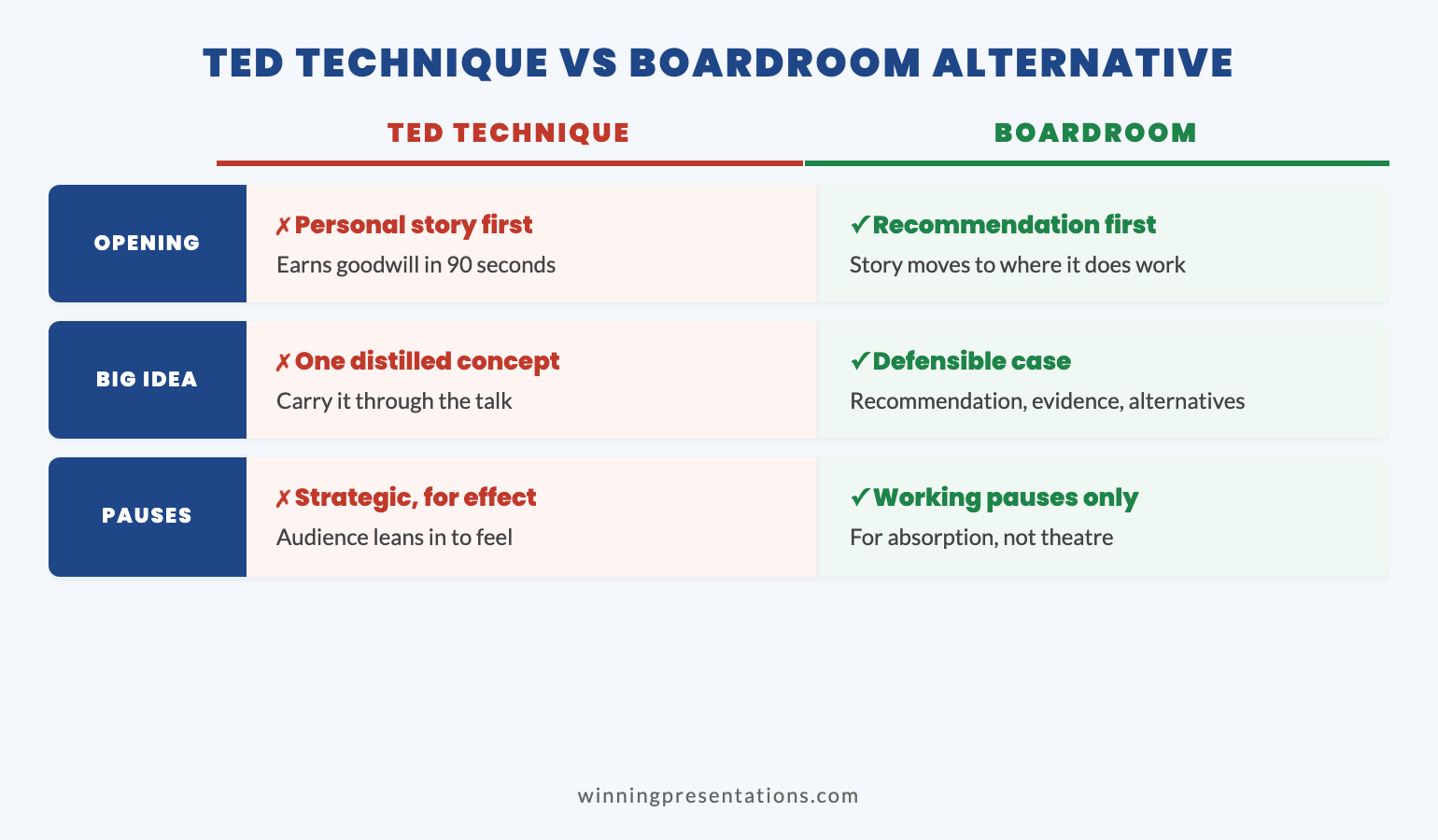
The course had not been a bad one. It had been a course built for someone else. The patterns it trained — opening lines, vocal warmth, story openings, eye contact across a wider audience — were the patterns of a keynote speaker. They were not the patterns of a divisional director answering a regulator’s question with the chair watching. The mismatch was not the course’s fault. It was a buying decision that had been made on rating rather than on fit.
This article is the framework Folake wishes she had used three weeks earlier — what a presenting with confidence course should and should not promise, and how to evaluate one before paying for it.
If senior-level rooms are where the nerves are loudest
Conquer Your Fear of Public Speaking is built around the patterns senior professionals face — committees, boards, regulators, investors — rather than generic stage fright. If that is the audience the course needs to fit, it is the right starting point.
What you are actually buying
The first piece of clarity worth having before paying for any presenting with confidence course is what the category actually contains. The phrase “confidence course” is doing a lot of work. It can mean a stage-fright recovery programme aimed at people whose nerves stop them speaking at all. It can mean a delivery polish programme aimed at trainers and speakers who already perform regularly. It can mean a senior-context programme aimed at directors, partners, and VPs who present rarely but in rooms where the cost of a wobble is high. These are three different products. The buying mistake most senior professionals make is treating them as interchangeable.
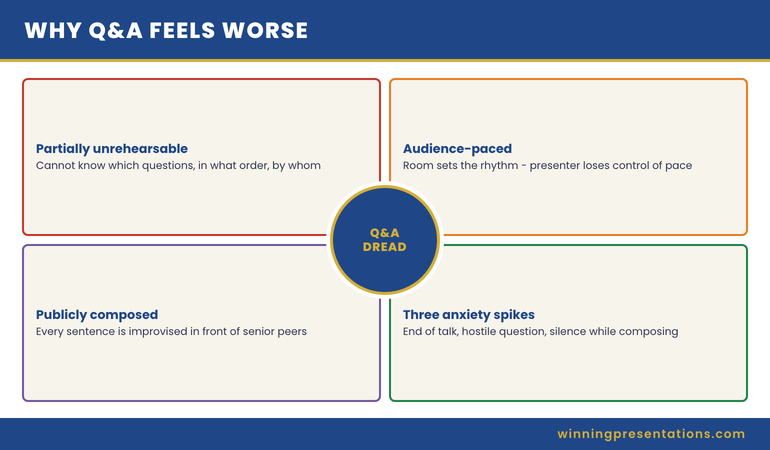
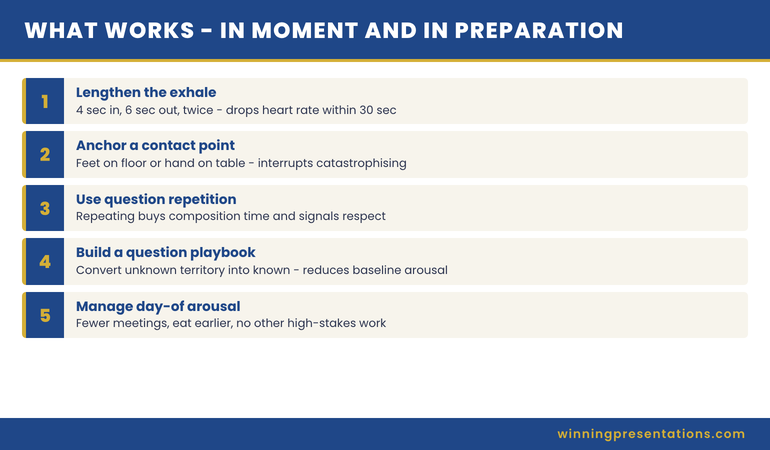
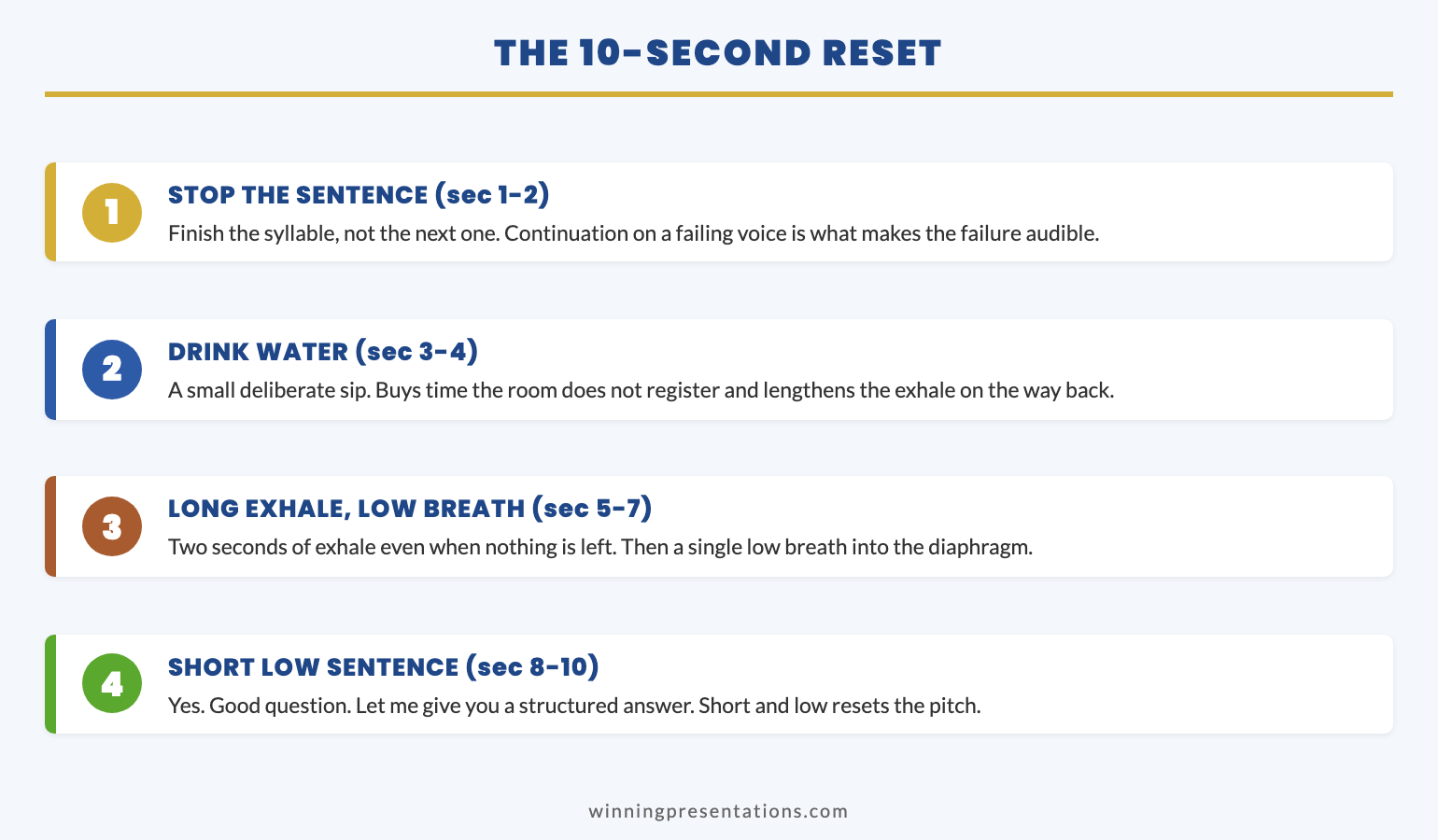
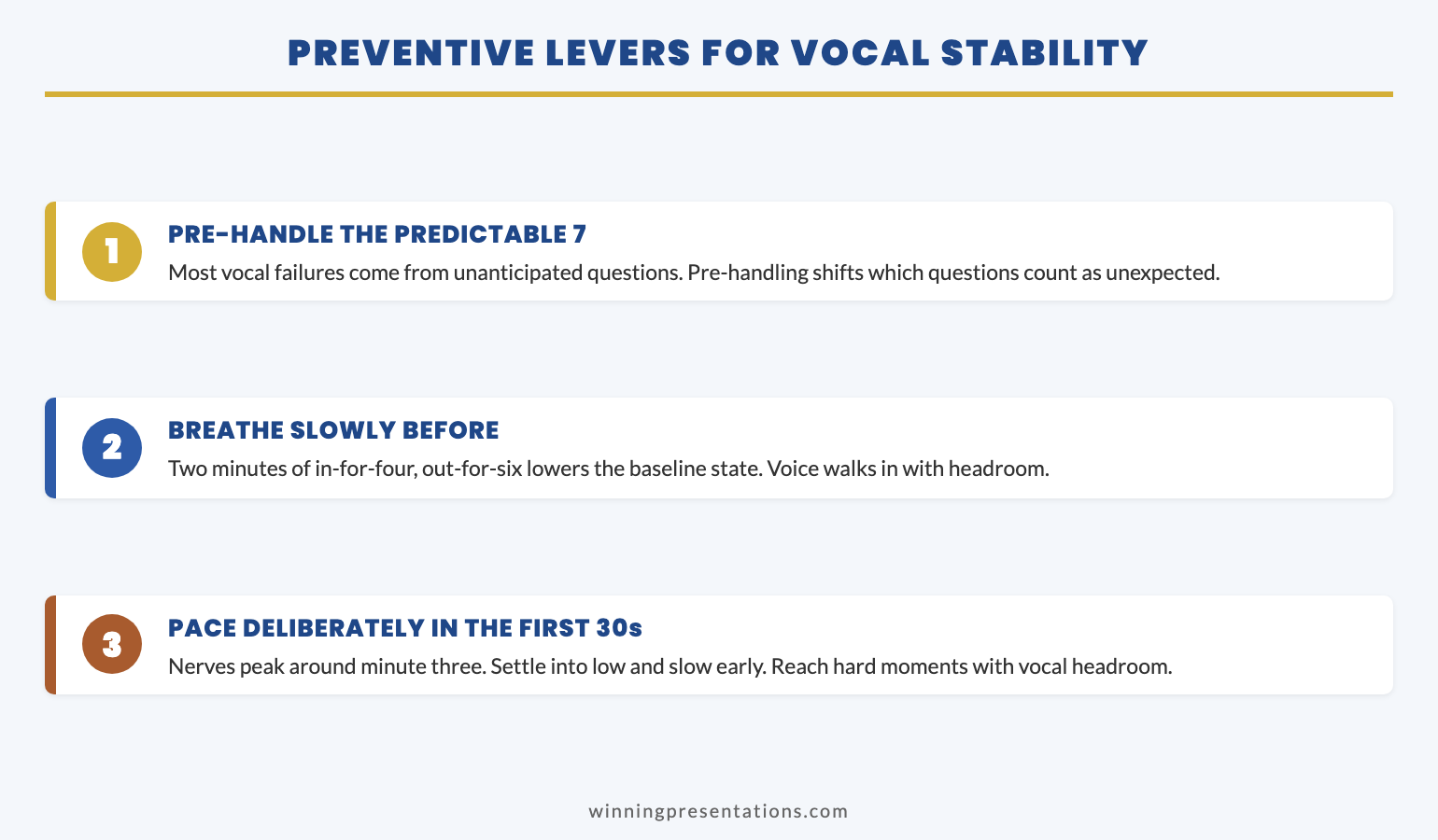
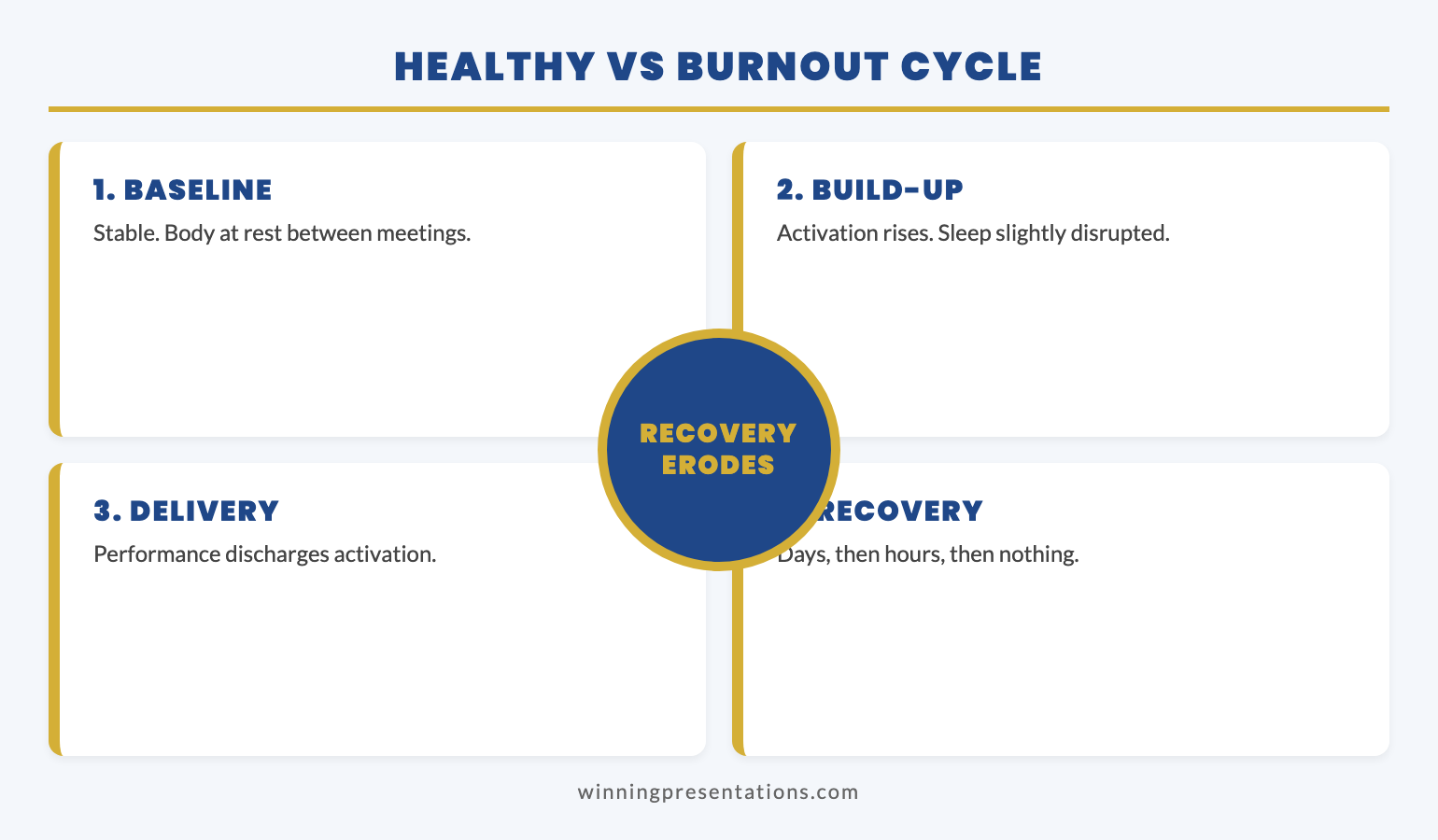
What a confidence course should promise is a specific body of training. Patterns for the audiences you actually face. Voice and breath techniques that hold up under pressure rather than only on a quiet stage. Recovery work for the moments where nerves show — a dry mouth, a quickening pace, a thought that loses its way mid-sentence. A confidence course should not promise that you will never feel nerves again, that the room will love you, or that approval will follow. Any course that promises any of those is selling something other than confidence.
The realistic outcome of a good confidence course is not the absence of nerves. It is the presence of patterns. Patterns the body and the voice can default to under pressure, so that the visible signs of nerves stop being read by the room as judgement signals. That distinction — patterns under pressure rather than freedom from pressure — is what separates a course that earns its price from a course that polishes the surface and leaves the underneath untouched.
Four dimensions to evaluate
A senior buyer should evaluate any presenting with confidence course online on four dimensions, in this order. Skipping the first is what produces the Folake result.
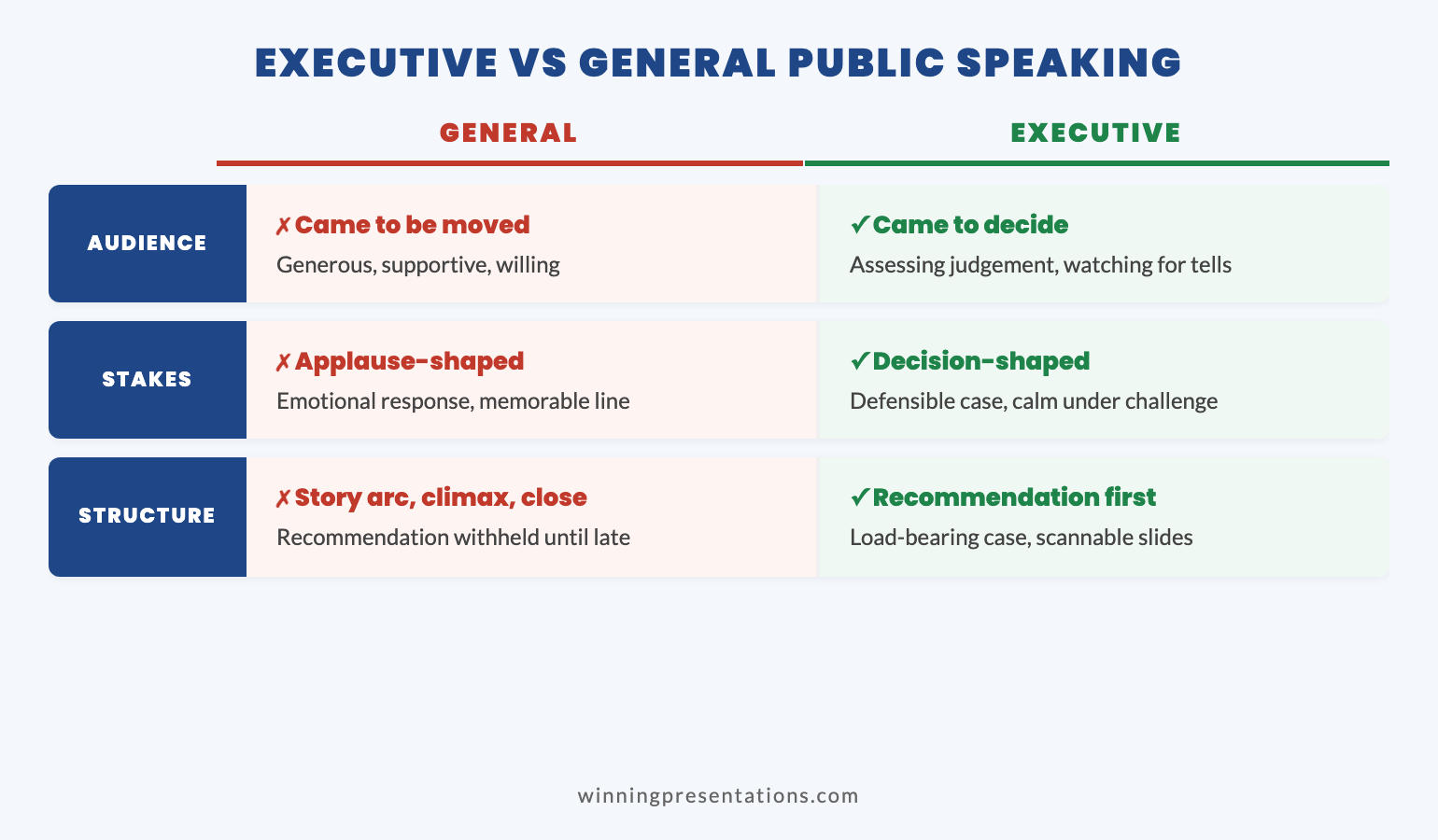
1. Audience fit. Who is the course built for? The marketing copy will rarely say this clearly, so look at the examples in the syllabus. If the case studies feature TEDx speakers, conference keynotes, sales kick-offs, or wedding speeches, the course is built for the keynote audience. If the case studies feature credit committees, board rooms, executive risk committees, regulator meetings, or investor pitches, the course is built for senior decision audiences. The same techniques can produce wildly different results in these two contexts. Audience fit is the dimension that decides whether the rest of the course transfers at all.
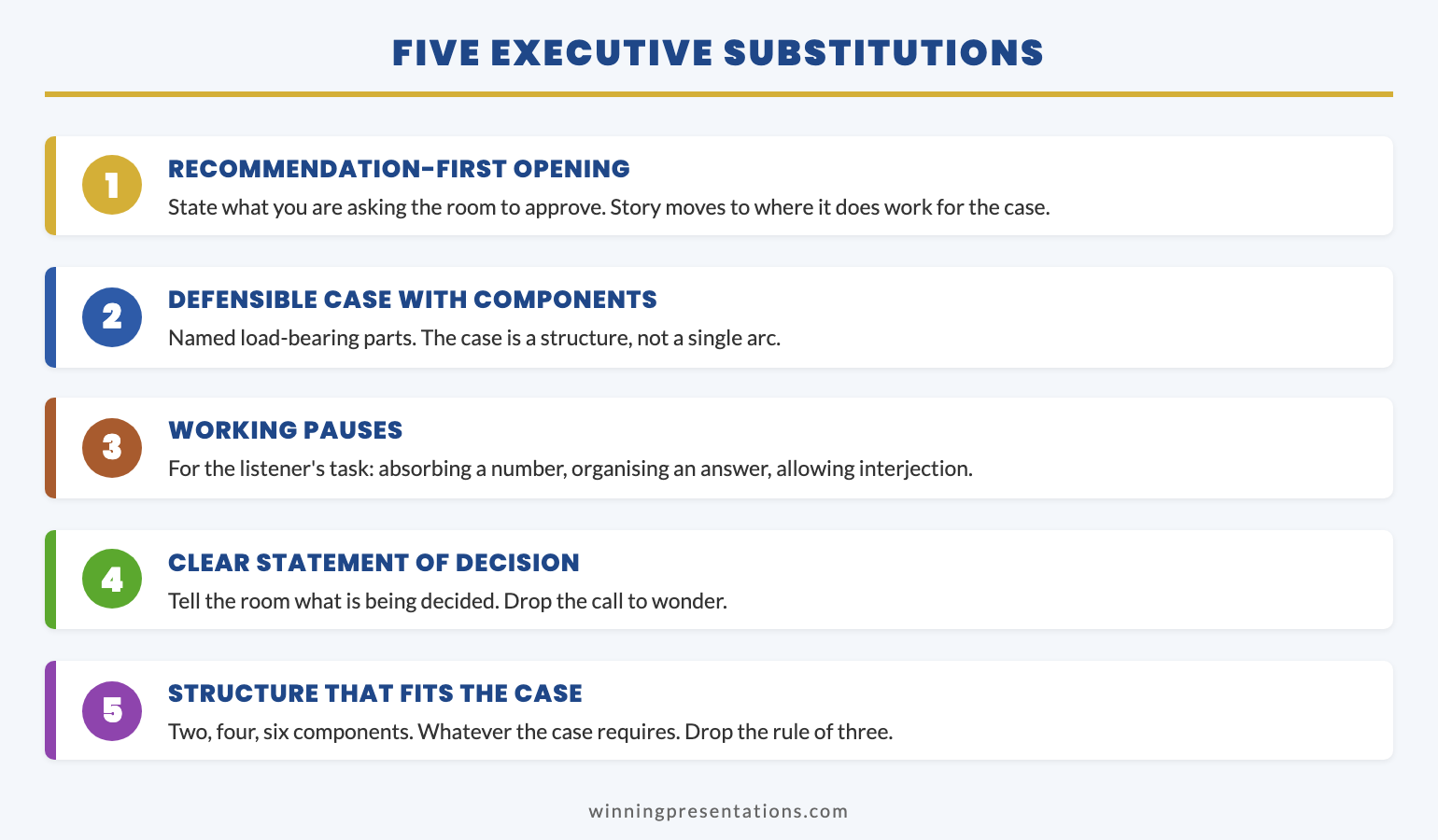
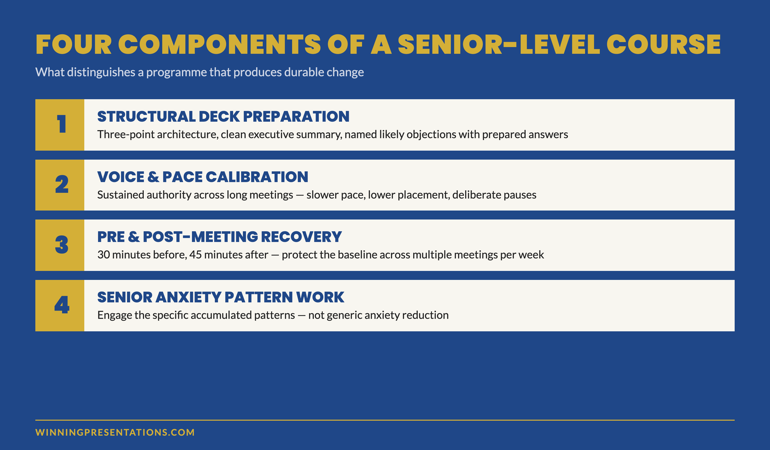
2. What is actually trained. Read the module list as a procurement memo. A confidence course built for senior contexts should spend most of its weight on calmness under scrutiny, voice and breath under pressure, and recovery from the visible signs of nerves. It should not spend most of its weight on opening lines, signature stories, or charismatic stage presence. Those are delivery skills. They are useful, but they are not what holds a senior professional together when a committee chair asks the difficult question. If the syllabus is mostly delivery polish, the course is a delivery polish course wearing a confidence label.
3. Format. Self-paced or cohort? Live or recorded? Both formats work — but they suit different buyers. A self-paced course suits a senior professional whose presenting calendar is irregular and who needs to revisit specific patterns before specific meetings. A cohort course suits someone who needs the accountability of a fixed schedule and a peer group. Neither is better in the abstract. The question is which fits the rhythm of your actual work. The wrong format is the second most common reason a confidence course fails to land, after audience mismatch.
4. Transfer to real rooms. The most important dimension and the one most courses cannot answer well. How does the work in the course transfer to the specific rooms you present in? A good confidence course will be specific about this. It will tell you which patterns are designed for short-form Q&A, which are designed for sustained presentations, and which are designed for the moments where nerves spike — the regulator’s first question, the chair’s interruption, the slide where the assumption is challenged. If the course cannot answer the transfer question, the work will stay in the course. It will not arrive in the room with you.
Red flags to watch for
A small set of patterns recurs across confidence courses that under-deliver for senior professionals. None of these are scams. They are simply mismatches that the marketing does not flag.
Clinical language without clinical depth. A confidence course is not a therapy programme. When the marketing leans heavily on words like “anxiety,” “phobia,” or “trauma” without the credentials and structure to back them up, the course is using clinical framing to sell a delivery skills product. Senior professionals rarely need clinical language. They need behavioural patterns that hold under pressure. The right framing for a senior buyer is calm, structured, and practical — not pathologised.
Generic stage-fright framing. If the course treats all nerves as the same nerve, it is built for general audiences. Senior-level nerves have a specific shape. They are situational, scrutiny-driven, and tied to credibility rather than to performance. A course that does not distinguish between general stage fright and senior-room scrutiny is a course built for someone else. The transfer to your real rooms will be partial at best.
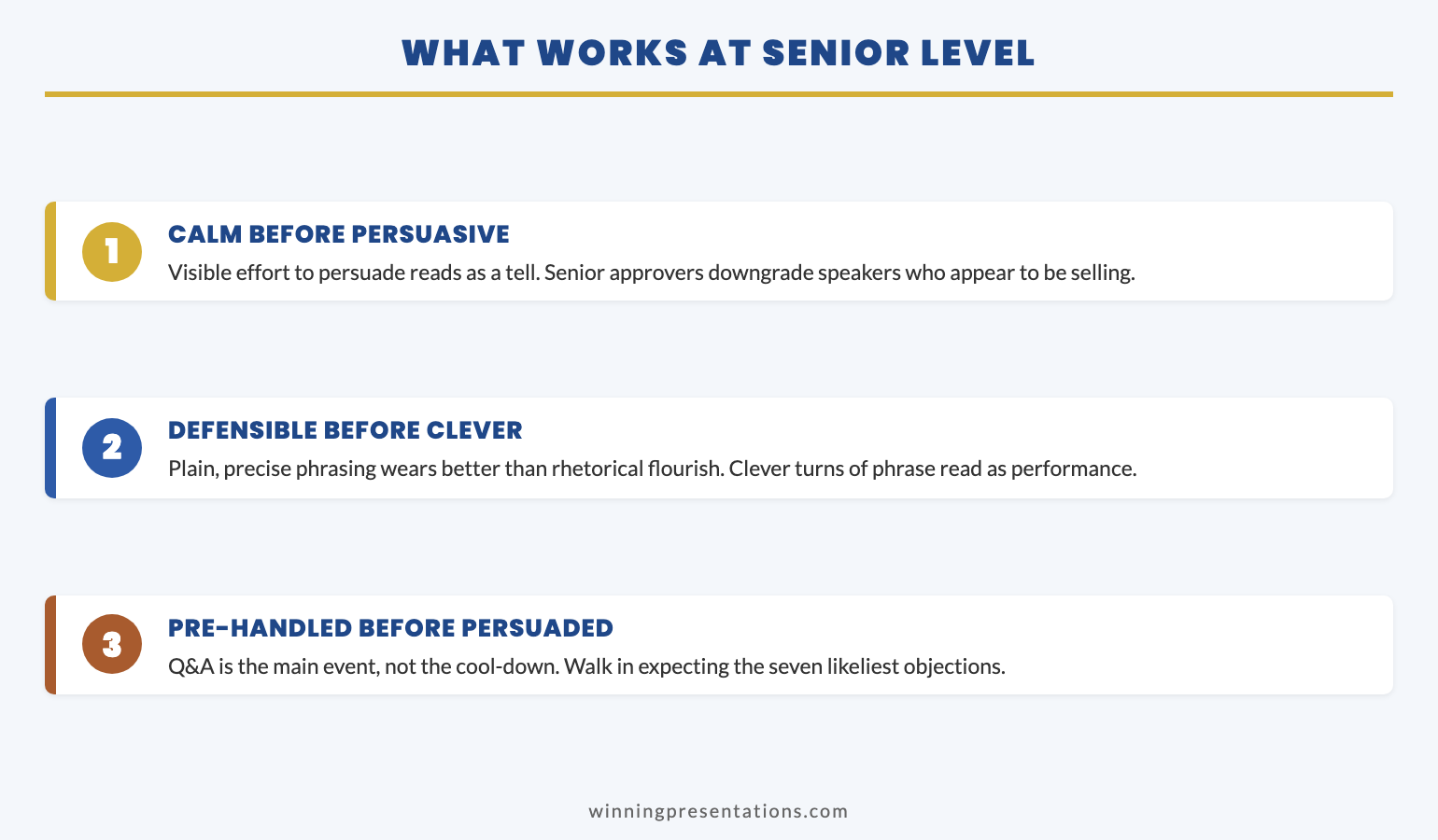
Big promises about outcomes. Any course that promises the room will love you, that approval will follow, or that nerves will disappear is selling outcomes the course cannot control. The honest promise of a confidence course is a process promise: better patterns under pressure, a calmer default voice, a clearer recovery from the moments where nerves show. Outcome promises are a marketing choice. Process promises are a professional one. Buy from the second.
This is similar to the due-diligence questions before paying for coaching — the same evaluation discipline applies whether you are paying for a course or for one-to-one work. The buyer who asks the structural questions first ends up with the better fit, almost regardless of the price point.
CONQUER YOUR FEAR OF PUBLIC SPEAKING
Built around the rooms senior professionals actually present in
A self-paced system addressing the specific patterns of senior-level public speaking nerves — calmness under scrutiny, voice and breath under pressure, and recovery techniques for the visible signs of nerves that read most loudly to senior audiences. Built for committees, boards, and regulator meetings rather than for keynote stages.
- Patterns for the specific audiences senior professionals face
- Structured techniques for the moments where nerves show most
- Voice, breath, and recovery work tied to executive scenarios
- Self-paced, instant access on purchase
Conquer Your Fear of Public Speaking — £39, instant access. Lifetime access to the materials.
Designed for senior-level decision audiences, not general stage performance.
What good looks like
A presenting with confidence course online that earns its place for a senior professional has a recognisable shape. The content is specific to the audience. The format respects the rhythm of senior work — short modules, clearly named, easy to revisit before a particular meeting rather than only consumable in one block. The promises are process promises, not outcome promises. The transfer to real rooms is named explicitly, with examples drawn from rooms that look like the buyer’s rooms.
Good also looks like restraint. A senior buyer should be wary of courses that promise to teach a complete public speaking system in a single product. The body of senior-level skill is wider than that. Confidence work is one strand. Slide structure is another. Stakeholder analysis is another. Case construction is another. A course that bundles everything tends to do none of it well. A course that is honestly scoped — “this is the confidence and delivery layer; the structural work is elsewhere” — tends to do its scope much better.
Good also includes what the course does not promise. It does not promise that nerves will disappear. It does not promise approval. It does not promise that the room will love you. It does not promise that the difficult question will not come. It promises patterns that hold under pressure when those things happen, which is the only honest promise a confidence course can make. The same discipline applies when senior professionals are weighing repeated rounds of training and asking whether they have hit training fatigue — restraint in the promise is what separates the course that earns repeat work from the one that exhausts the buyer.
If you are evaluating where the confidence work fits within a wider professional toolkit, professional public speaking training online is the natural next reference. It walks through how confidence training, delivery training, and structural training fit together — and which to buy first depending on the room you most often present in.
Making the decision
The buying decision for a presenting with confidence course online comes down to one question that contains all four evaluation dimensions: does this course train the specific patterns of the rooms I actually present in? If the answer is yes, the course is likely to transfer. If the answer is “I am not sure, but it is highly rated,” the course is likely to leave you, like Folake, more polished but no calmer.
For senior professionals — directors, VPs, partners, regulators’ counterparts — the rooms in question are decision rooms, not applause rooms. The audiences are reading you as a colleague being assessed rather than as a speaker being supported. The nerves that show up in those rooms are a specific kind of nerve. They are not solved by a stage-presence programme. They are not solved by storytelling. They are solved by patterns built for scrutiny — calm voice, controlled breath, a recovery from the moments where the body wants to speed up. The course that trains those patterns is the course worth buying. The one that does not, is not, regardless of price or rating.
Most senior professionals who go through this evaluation arrive at the same shortlist: a self-paced system that respects an irregular calendar, scoped specifically to confidence and delivery rather than the whole curriculum, and built around senior decision audiences rather than general stage performance. That shortlist is short by design — most courses on the open market do not meet all three criteria. The ones that do are the ones worth paying for. A speaking confidence course built for professionals applies the same evaluation lens, with side-by-side comparisons of the typical course types.
This is the same buying discipline that applies to other senior development decisions — see the presentation skills gap at VP level for a parallel framework on how to evaluate fit before paying for any senior-context training.
CONQUER YOUR FEAR OF PUBLIC SPEAKING
Self-paced, instant access, lifetime to the materials
Buy once, keep the materials, revisit before specific meetings. The structured techniques, voice and breath work, and recovery patterns are organised for the irregular rhythm of senior presenting calendars — not for a fixed-week cohort schedule. £39, instant access.
For senior professionals who present rarely but in rooms where calmness matters most.
Frequently asked questions
What should a presenting with confidence course online actually contain?
For senior professionals, the core content should be calmness under scrutiny, voice and breath under pressure, and recovery techniques for the visible signs of nerves. Delivery polish — opening lines, stage presence, vocal warmth — is useful but secondary. The test is whether the syllabus addresses the specific audiences and rooms the buyer presents in, rather than treating all public speaking nerves as the same nerve. A course built for keynote stages will transfer only partially to a credit committee or a board.
Is a self-paced course better than a live cohort for confidence work?
Neither format is better in the abstract. A self-paced course suits a senior professional whose presenting calendar is irregular — the kind who needs to revisit a specific pattern in the week before a particular meeting. A live cohort suits a buyer who needs the accountability of a fixed schedule and a peer group. The mistake is buying the format that fits someone else’s rhythm. Match the format to the actual rhythm of your presenting work.
What red flags should I watch for when evaluating a course?
Three recur. Clinical language (“anxiety,” “phobia,” “trauma”) without the credentials to back it up — that signals a delivery course wearing a clinical label. Generic stage-fright framing that treats all nerves as the same nerve — that signals a course built for general audiences. And outcome promises that the room will love you or approval will follow — those are promises a course cannot keep. The honest promises a confidence course can make are process promises about patterns under pressure.
How long should a presenting with confidence course take to complete?
For a senior buyer, the question is less about total length and more about modular structure. A course that can only be consumed in one block does not fit how senior professionals actually use this material — they revisit specific patterns before specific meetings rather than working straight through. A well-designed self-paced confidence course will have short, clearly named modules so a particular pattern (recovering from a difficult question, controlling pace under pressure) can be re-watched in fifteen minutes the night before a presentation.
The Winning Edge
A weekly newsletter for senior professionals who present at board level. One specific structural idea per issue, drawn from real boardroom and committee work. No filler.
Not ready for the full system? Start here instead: download the free Executive Presentation Checklist — the pre-flight checks that catch the structural mistakes most senior professionals make in the last 24 hours before a high-stakes meeting.
If this article landed for you, How to build confidence in public speaking is the natural next read. It walks through the practical patterns senior professionals use to build calmness under scrutiny, with examples drawn from the same kinds of rooms.
Next step: open the syllabus of any presenting with confidence course you are considering and run the four-dimension check — audience fit, what is actually trained, format, and transfer to your real rooms. If any of the four is unclear from the marketing copy, that is the question to ask before buying. Most buyers skip the first dimension and pay for the consequences.
Mary Beth Hazeldine is the Owner & Managing Director of Winning Presentations. With 24 years of corporate banking experience at JPMorgan Chase, PwC, Royal Bank of Scotland, and Commerzbank, she advises senior professionals across financial services, healthcare, technology, and government on structuring presentations for high-stakes funding rounds and approvals. She speaks German and works extensively with the German-speaking financial markets.