
When Public Speaking Fear Becomes a Medical Emergency: Signs You Need More Than Techniques
I kept beta blockers in my desk drawer for three years.
Never took one. But knowing they were there — knowing I had an exit — was the only thing that got me into some meeting rooms on bad days. The shaking, the nausea, the voice that cracked regardless of how many times I’d rehearsed. I had all of it. For five years before I found what actually worked.
What I’ve learned since, from training thousands of executives, is that there’s a line most people don’t know how to find. On one side: normal performance anxiety that techniques can fix. On the other: something that has crossed into the nervous system so deeply that breathing exercises and positive self-talk aren’t touching it.
This article is for people who suspect they might be on the wrong side of that line.
Quick answer: Public speaking anxiety becomes a medical concern when it produces physical symptoms that are disproportionate, persistent, and interfering with professional function — vomiting, chest pain, blackouts, or days of anticipatory dread before a single meeting. These are signs the nervous system is operating in a trauma response, not just a performance stress response. Standard presentation techniques don’t reach this level. What does: nervous system regulation work, clinical-grade somatic techniques, and in some cases, medical consultation for anxiety disorders or specific phobia.
🚨 Have a presentation this week and physical symptoms are already starting? Calm Under Pressure (£19.99) is built specifically for in-the-moment physical symptom management — the 60-second resets for shaking, nausea, racing heart, and voice cracking, for the day of the presentation.
Jump to:
A C-suite executive I worked with had a secret she’d kept for three years.
She vomited before every major presentation. Not occasionally. Every single time, without exception, for three years. Her team thought she was one of the most composed presenters in the company. She had a 20-minute window in the bathroom before each meeting and a very precise mental ritual for walking back in as though nothing had happened.
She was referred to me after an incident that finally scared her: she blacked out briefly in the lift on the way to a board presentation. Came to in time, walked in, delivered the presentation. Nobody knew. But she knew.
That’s when we crossed from “I get nervous” into a different conversation entirely.
She didn’t need better techniques. She needed nervous system work that addressed what was actually happening in her body — not a list of tips for managing nerves. The techniques she’d tried for years hadn’t failed her because she hadn’t tried hard enough. They’d failed because they weren’t designed for what she was experiencing.
Normal Presentation Nerves vs. Medical Emergency: What’s the Difference?
Some level of performance anxiety is physiologically normal. The autonomic nervous system interprets high-stakes visibility — standing in front of people who are evaluating you — as a threat signal. Heart rate increases. Cortisol rises. Muscle tension increases. That’s not malfunction. That’s your body trying to help.
What makes anxiety cross into concerning territory isn’t the presence of those symptoms. It’s the severity, the duration, and the functional impairment.
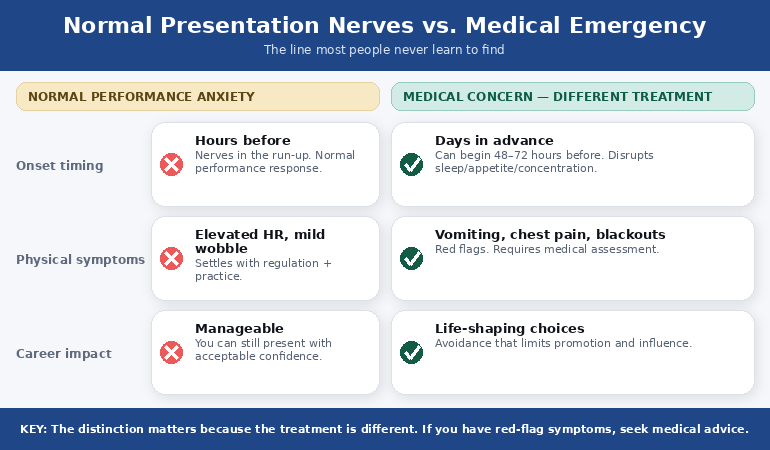
Normal performance anxiety: you feel nervous in the hours before a presentation. Your heart rate is elevated when you stand up to speak. Your voice might wobble slightly at the start. Within the first 60–90 seconds, the nervous system regulation kicks in and you settle.
Concerning anxiety: the dread starts days in advance. Physical symptoms — nausea, gastrointestinal distress, sleep disruption — begin 24–72 hours before the presentation. On the day, symptoms reach a level that impairs function: shaking that you can’t stop, voice loss, blanking on content you’ve rehearsed dozens of times, or physical symptoms severe enough to affect your health (vomiting, chest pain, difficulty breathing, pre-syncope or blackouts).
The distinction matters because the treatment is different. Techniques designed for normal performance anxiety — breathing exercises, visualisation, anchoring, positive self-talk — operate at the cortical level. They work on the thoughts. When anxiety is operating at the level of a trauma or phobia response, the threat signal is firing from subcortical brain structures that don’t respond to reasoning or intention. You can’t think your way out of a nervous system response that’s running below conscious control.
🧠 The 60-Second Resets That Stop Physical Symptoms Before They Take Over
Calm Under Pressure is built specifically for in-the-moment physical symptom management on presentation day — not theory, not mindset tips. The techniques from clinical hypnotherapy and NLP, adapted for high-pressure executive environments:
- The 60-second nervous system reset for racing heart, shaking, or voice cracking — designed to be used in the corridor outside the meeting room
- The pre-meeting vomiting and nausea protocol — specific techniques for gastrointestinal anxiety responses before high-stakes presentations
- The voice recovery sequence — what to do when your voice cracks or tightens in the first 90 seconds
- The blank-mind recovery technique — how to retrieve content your brain has temporarily blocked under threat response
- The grounding sequence for dissociation and pre-syncope — for those who experience derealization or lightheadedness before presenting
Get Calm Under Pressure → £19.99
Evidence-based techniques from clinical hypnotherapy and NLP, adapted for executive environments. Used by presenters who had tried everything else first.
The Symptoms That Cross the Line
There is no single threshold, because individual nervous systems vary. But certain presentations of anxiety warrant medical assessment rather than (or in addition to) technique-based intervention:
Cardiovascular symptoms. Chest tightness, palpitations, or irregular heartbeat before or during a presentation should always be checked medically first, before attributing them to anxiety. The anxiety interpretation may be correct — but ruling out cardiac causes is not optional.
Pre-syncope or blackouts. Lightheadedness, tunnel vision, or actual loss of consciousness connected to presentation situations is a medical symptom. This can have anxiety-related causes (vasovagal syncope is common in high-stress situations) but it needs assessment.
Severe gastrointestinal distress. Vomiting before every presentation for months, or persistent gastrointestinal symptoms that begin days in advance and don’t resolve, may indicate a physiological anxiety disorder rather than a situational one. This is different from occasional nausea on a particularly high-stakes day.
Anticipatory dread lasting days. When anxiety about a presentation begins 48–72 hours in advance and is functionally impairing — disrupting sleep, appetite, or concentration on unrelated work — that’s a level of anticipatory anxiety that clinical intervention is designed for. Breathing exercises don’t reach anticipatory anxiety that’s already running three days ahead.
Avoidance that’s costing career opportunities. This is perhaps the most common threshold that goes unnamed. When a professional is declining presentations, turning down visibility, or shaping their entire career choices around avoiding public speaking — that’s a level of interference that warrants taking seriously. It doesn’t have to be dramatic symptoms. Chronic, career-shaping avoidance is its own form of severity.
For more on how the nervous system gets stuck in presentation trauma patterns, this article is relevant background: Presentation Trauma and the Nervous System.
Recognise any of those symptoms? Calm Under Pressure handles the in-the-moment physical responses — the ones that techniques like breathing exercises and visualisation don’t reach quickly enough on presentation day.
Why Standard Techniques Stop Working at This Level
Most presentation anxiety advice — and most presentation coaches — operates at the behavioural level. Practice more. Breathe. Visualise success. Reframe your thoughts. These are legitimate techniques, and they work for a significant proportion of people with normal-range performance anxiety.
They don’t work when the anxiety has become a conditioned response. That’s the clinical distinction most presentation advice ignores.
A conditioned response is what happens when the nervous system has encoded “presentation” as a threat signal through repeated experience. You’ve presented while anxious. The anxiety was uncomfortable. The nervous system noted the correlation: presentation environment = threat. This encoding happens below conscious awareness — which is why telling yourself “there’s nothing to be afraid of” doesn’t change the physical response. The part of your brain generating the response doesn’t speak the language of rational reassurance.
The C-suite executive who vomited before every board meeting had been practising breathing techniques for two years before she came to me. The techniques weren’t wrong. They were just operating on the wrong part of the nervous system. When we shifted to somatic work — approaches that address the conditioned response directly through the body rather than through reasoning — the physical symptoms resolved in six weeks of consistent practice. Not years. Six weeks.
That’s the difference between treating the symptom and treating the signal. Standard techniques treat the symptom. Somatic and clinical approaches treat the signal — the nervous system’s learned association between presentation contexts and threat. You can’t always do deep somatic work on the day of a presentation. For in-the-moment management, you need a different set of tools. For the underlying pattern, you need to go deeper.
If you’ve tried the standard approaches and they haven’t worked, this is directly relevant: Treatment-Resistant Presentation Anxiety — What’s Actually Left to Try.
What Actually Works When Techniques Don’t
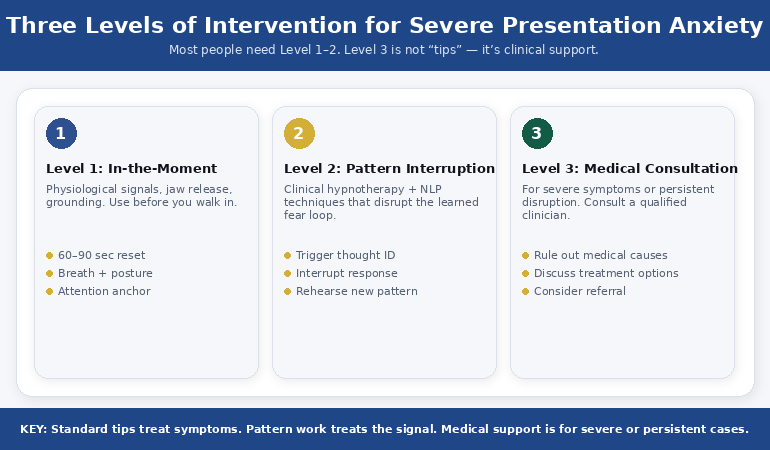
There are three levels of intervention for severe presentation anxiety, and the right one depends on what’s driving the symptoms.
Level 1: In-the-moment symptom management. For physical symptoms on the day — shaking, nausea, voice cracking, heart racing — somatic techniques work faster than cognitive ones. Physiological sighing (double inhale through the nose, extended exhale) reduces heart rate measurably within 60 seconds and doesn’t require sustained practice to work. Cold water on the wrists, jaw release, and specific grounding sequences address the physical presentation of the response rather than the thought behind it. These are the tools that work in the corridor outside the meeting room when you have 90 seconds and nowhere to hide.
Level 2: Pattern interruption. For anticipatory anxiety that begins days in advance, the intervention needs to work on the conditioned association rather than just the acute response. Techniques from clinical hypnotherapy and NLP — specifically those that work on the encoded memory structures behind the conditioned response — are effective here. This is where I do most of my individual client work. The executive who vomited before every board meeting saw resolution at this level: the acute response in the meeting room resolved once the underlying conditioned association was disrupted.
Level 3: Medical consultation. For symptoms that include chest pain, blackouts, or a level of impairment that’s affecting quality of life beyond presentation situations, medical assessment is appropriate. A GP can evaluate for specific phobia or social anxiety disorder, refer to a CBT or EMDR specialist, and assess whether medication is a useful adjunct (not a replacement) for the work above. There is no shame in this. There is also no award for suffering through a diagnosable condition without support.
Most people reading this need Level 1 and Level 2 — not a medical referral, but also not the standard advice they’ve already tried. The in-the-moment work and the pattern-interruption work are the gap between “I’ve tried everything” and “I’ve actually tried the right things.”
🛑 Stop Relying on Techniques That Were Never Designed for Severe Physical Symptoms
- The clinical somatic techniques for in-the-moment management of shaking, nausea, heart racing, and voice cracking — designed for executive environments, not therapy rooms
- The pre-meeting protocol for the morning of a high-stakes presentation when physical symptoms are already escalating
Get Calm Under Pressure → £19.99
Created by a qualified clinical hypnotherapist with 5 years of her own severe presentation anxiety — and 24 years watching executives face it in the highest-stakes rooms in global banking.
PAA: Quick Answers on Severe Presentation Anxiety
Is it normal to vomit before a presentation?
Occasional nausea before a very high-stakes presentation is within the range of normal performance anxiety. Vomiting before most or every significant presentation is not — it indicates a level of physiological activation that warrants clinical attention rather than more breathing exercises. This is a conditioned response, not weakness. It’s treatable.
Can presentation anxiety cause chest pain?
Yes — anxiety activates the cardiovascular system and can cause chest tightness, palpitations, and discomfort that mimics cardiac symptoms. However, chest pain should always be medically evaluated before attributing it to anxiety. This is non-negotiable. Once a cardiac cause is ruled out, anxiety-related chest symptoms respond well to somatic regulation techniques and, in persistent cases, clinical anxiety treatment.
I’ve tried everything for presentation anxiety. What’s left?
Usually the missing piece is the level of intervention, not the category. Most people have tried behavioural techniques (breathing, practice, visualisation) but haven’t worked at the somatic level — techniques that address the conditioned nervous system response directly rather than through reasoning. If you’ve tried techniques without sustained success, the panic attack before presentation framework explains the next level of what’s available.
Is Calm Under Pressure Right For You?
✔️ This is for you if:
- You experience physical symptoms — shaking, nausea, voice cracking, racing heart — on presentation day and need something that works fast, in the moment
- You’ve tried breathing exercises and standard anxiety techniques and they’re not enough on a high-stakes day
- You have an upcoming presentation and want clinical-grade in-the-moment tools, not more theory
❌ This is NOT for you if:
- Your challenge is the underlying anxiety pattern over months and years rather than acute day-of symptoms — for that level, Conquer Speaking Fear (£39) addresses the root cause rather than the in-the-moment response
- Your presenting challenge is slide structure rather than anxiety — for that, see today’s executive slide structure article
If you recognised your own experience in the severe end of what’s described above, the gap isn’t willpower or more practice. It’s having the right intervention at the right level — clinical tools designed for the body’s response, not the mind’s.
🧪 Clinical Tools for Physical Symptoms — Built From 5 Years of My Own
I spent five years with the full range of physical presentation anxiety: nausea, shaking, voice cracking, face flushing. I also have clinical hypnotherapy and NLP qualifications. Calm Under Pressure is what I wish I’d had in those years — not theory, not motivation, but the specific techniques that address what the body is actually doing:
- In-the-moment resets for every major physical symptom: shaking, nausea, voice cracking, racing heart, facial flushing, mind going blank
- The pre-meeting morning protocol — what to do from the moment you wake up on a high-stakes presentation day
- The 90-second grounding sequence for dissociation and lightheadedness
- The vomiting and gastrointestinal anxiety protocol — the techniques I developed specifically because this symptom is almost never addressed anywhere else
- Voice recovery techniques — somatic resets for tightening or cracking that work in the first 90 seconds of a presentation
Get Calm Under Pressure → £19.99
Your next presentation is already on your calendar. The symptoms are not going to resolve on their own. Get the tools that actually work for severe physical anxiety — on the day you need them.
Frequently Asked Questions
How do I know if my presentation anxiety needs professional help?
The thresholds to watch for: physical symptoms that are severe (vomiting, blackouts, chest pain), anticipatory dread that starts days in advance and disrupts your functioning, or career-shaping avoidance where you’re turning down opportunities because of the anxiety. Any of these warrant taking more seriously than standard self-help techniques. Starting with your GP is appropriate if you’re experiencing cardiovascular or other concerning physical symptoms. For anxiety that’s functioning but severe, a clinical hypnotherapist, CBT therapist, or EMDR practitioner who specialises in performance anxiety is a good route.
Are beta blockers effective for public speaking anxiety?
Beta blockers reduce the cardiovascular manifestations of anxiety — heart racing, trembling, voice shake — but they don’t address the underlying anxiety itself. They can be useful as a short-term bridge when the physical symptoms are impairing function and nothing else is working quickly enough. They are not a treatment for the conditioned anxiety pattern. Most people I work with who have used beta blockers find them less effective than they expected, or find they create a dependency on having them available (as I described with having them in my desk drawer) rather than actually resolving the problem.
Can presentation anxiety get worse over time even if I keep presenting?
Yes — this is counterintuitive but important. The standard advice is “present more, fear less.” For many people, this is true. For others, repeated experiences of presenting while highly anxious don’t reduce the anxiety — they reinforce the conditioned association. Every high-anxiety presentation can deepen the nervous system’s encoding of “presentation = threat.” This is why some people find their anxiety gets worse through their careers despite years of presenting regularly. More exposure isn’t the answer if the exposure is consistently aversive. The pattern needs interrupting, not reinforcing.
I have a board presentation in two weeks. What should I do right now?
Start with the in-the-moment physical tools — the grounding, breathing, and voice reset techniques that you can practise now and use on the day. These take two to three days of daily practice to work reliably under pressure. Don’t start them on the morning of the presentation. Alongside that, work on the preparation side — a well-structured deck reduces anxiety because it removes uncertainty about what comes next. For structure, see the due diligence presentation framework if it’s a high-stakes investor context, or the hypothetical questions framework if you’re anticipating a tough Q&A.
📊 Want better slides too?
Preparation reduces anxiety. The Executive Slide System (£39) includes confident-presenter templates designed to minimise preparation stress — so you walk into the room knowing the structure works, not hoping it does.
📬 The Winning Edge — Weekly Presentation Intelligence
One article per week on executive communication, presentation anxiety, and high-stakes performance. Evidence-based, executive-focused, no fluff.
🆓 Free resource: 7 Presentation Frameworks — a free guide to strengthen your presentation preparation.
Also published today: if your challenge is the slide structure for a high-stakes presentation rather than the anxiety, see The Due Diligence Presentation That Almost Killed a £50M Deal. And if you’re preparing for executive Q&A with difficult hypothetical questions, read The Hypothetical Trap.
About the Author
Mary Beth Hazeldine is the Owner & Managing Director of Winning Presentations. With 24 years of corporate banking experience at JPMorgan Chase, PwC, Royal Bank of Scotland, and Commerzbank, she has delivered high-stakes presentations in boardrooms across three continents.
A qualified clinical hypnotherapist and NLP practitioner, Mary Beth combines executive communication expertise with evidence-based techniques for managing presentation anxiety. She has trained thousands of executives and supported presentations for high-stakes funding rounds and approvals.